DNA STRUCTURE
The Structure of the DNA Molecule
Access Excellence Classic Collection
--------------------------------------------------------------------------------
Background
Although scientists as far back in history as Aristotle recognized that the features of one generation are passed on to the next (...like begets like...) it was not until the 1860's that the fundamental principles of genetic inheritance were described by Gregor Mendel. Mendel's work with common garden peas, pisum sativum, led him to hypothesize that phenotypic traits (physical characteristics) are the result of the interaction of discrete particles, which we now call genes, and that both parents provide particles which make up the characteristics of the offspring. His theories were, however, widely disregarded by scientists of the time. In the last quarter of the 19th century, however, microscopists and cytologists, interested in the process of cell division, developed both the equipment and the methods needed to visualize chromosomes and their division in the processes of mitosis (A. Schneider, 1873) and of meiosis (E. Beneden, 1883).
As the 20th century began many scientists noticed similarities in the theoretical behavior of Mendel's particles, and the visible behavior of the newly discovered chromosomes. It wasn't long before most scientists were convinced that the hereditary material responsible for giving living things their characteristic traits, and chromosomes must be one in the same. Yet, questions still remained. Chemical analysis of chromosomes showed them to be composed of both protein and DNA. Which substance carried the hereditary information? For many years most scientists favored the hypothesis that protein was the responsible molecule because of its comparative complexity when compared with DNA. After all, DNA is composed of a mere 4 subunits while protein is composed of 20, and DNA molecules are linear while proteins range from linear to multiply branched to globular. It appeared clear that the relatively simple structure of a DNA molecule could not carry all of the genetic information needed to account for the richly varied life in the world around us!
It was not until the late 1940's and early 1950's that most biologists accepted the evidence showing that DNA must be the chromosomal component that carries hereditary information. One of the most convincing experiments was that of Alfred Hershey and Martha Chase who, in 1952, used radioactive labeling to reach this conclusion(See Graphics). This team of biologists grew a particular type of phage, known as T2, in the presence of two different radioactive labels so that the phage DNA incorporated radioactive phosphorus (32P), while the protein incorporated radioactive sulfur (35S). They then allowed the labeled phage particles to infect non-radioactive bacteria and asked a very simple question: which label would they find associated with the infected cell? Their analysis showed that most of the 32P-label was found inside of the cell, while most of the 35S was found outside. This suggested to them that the proteins of the T2 phage remained outside of the newly infected bacterium while the phage-derived DNA was injected into the cell. They then showed that the phage derived DNA caused the infected cells to produce new phage particles. This elegant work showed, conclusively, that DNA is the molecule which holds genetic information. Meanwhile, much of the scientific world was asking questions about the physical structure of the DNA molecule, and the relationship of that structure to its complex functioning.
Watson and Crick
In 1951, the then 23-year old biologist James Watson traveled from the United States to work with Francis Crick, an English physicist at the University of Cambridge. Crick was already using the process of X-ray crystallography to study the structure of protein molecules. Together, Watson and Crick used X-ray crystallography data, produced by Rosalind Franklin and Maurice Wilkins at King's College in London, to decipher DNA's structure.
This is what they already knew from the work of many scientists, about the DNA molecule:
DNA is made up of subunits which scientists called nucleotides.
Each nucleotide is made up of a sugar, a phosphate and a base.
There are 4 different bases in a DNA molecule:
adenine (a purine)
cytosine (a pyrimidine)
guanine (a purine)
thymine (a pyrimidine)
The number of purine bases equals the number of pyrimidine bases
The number of adenine bases equals the number of thymine bases
The number of guanine bases equals the number of cytosine bases
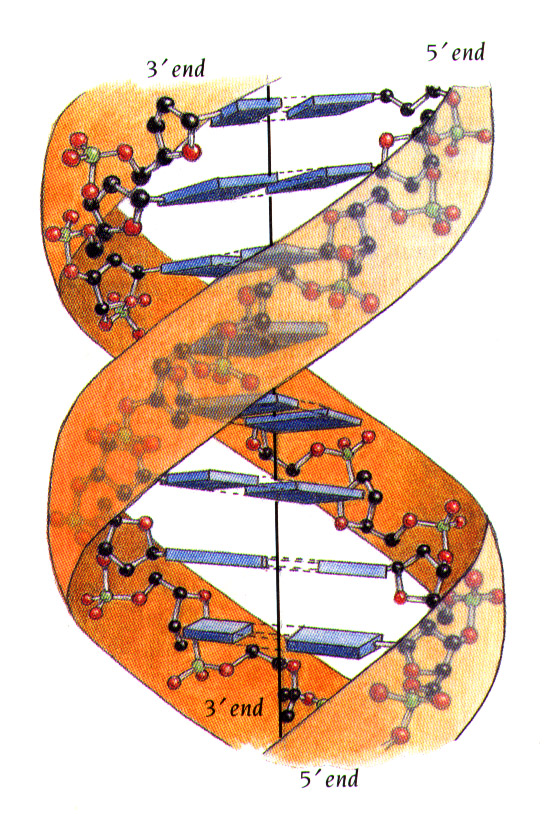
The basic structure of the DNA molecule is helical, with the bases being stacked on top of each other
Working with nucleotide models made of wire, Watson and Crick attempted to put together the puzzle of DNA structure in such a way that their model would account for the variety of facts that they knew described the molecule. Once satisfied with their model, they published their hypothesis, entitled "Molecular Structure of Nucleic Acids: A Structure for Deoxyribose Nucleic Acid" in the British journal Nature (April 25, 1953. volume 171:737-738.) It is interesting to note that this paper has been cited over 800 times since its first appearance!
Here are their words:
"...This (DNA) structure has two helical chains each coiled round the same axis...Both chains follow right handed helices...the two chains run in opposite directions. ..The bases are on the inside of the helix and the phosphates on the outside..."
"The novel feature of the structure is the manner in which the two chains are held together by the purine and pyrimidine bases... The (bases) are joined together in pairs, a single base from one chain being hydrogen-bonded to a single base from the other chain, so that the two lie side by side...One of the pair must be a purine and the other a pyrimidine for bonding to occur. ...Only specific pairs of bases can bond together. These pairs are: adenine (purine) with thymine (pyrimidine), and guanine (purine) with cytosine (pyrimidine)."
"...in other words, if an adenine forms one member of a pair, on either chain, then on these assumptions the other member must be thymine; similarly for guanine and cytosine. The sequence of bases on a single chain does not appear to be restricted in any way. However, if only specific pairs of bases can be formed, it follows that if the sequence of bases on one chain is given, then the sequence on the other chain is automatically determined."
and
"...It has not escaped our notice that the specific pairing we have postulated immediately suggests a possible copying mechanism for the genetic material."
And with these words, the way was made clear for tremendous strides in our understanding of the structure of DNA and, as a result our ability to work with and manipulate the information-rich DNA molecule.
|
 |
Genes, which are carried on chromosomes, are the basic physical and functional units of heredity. Genes are specific sequences of bases that encode instructions on how to make proteins. Although genes get a lot of attention, it’s the proteins that perform most life functions and even make up the majority of cellular structures. When genes are altered so that the encoded proteins are unable to carry out their normal functions, genetic disorders can result.
Gene therapy is a technique for correcting defective genes responsible for disease development. Researchers may use one of several approaches for correcting faulty genes:
A normal gene may be inserted into a nonspecific location within the genome to replace a nonfunctional gene. This approach is most common.
An abnormal gene could be swapped for a normal gene through homologous recombination.
The abnormal gene could be repaired through selective reverse mutation, which returns the gene to its normal function.
The regulation (the degree to which a gene is turned on or off) of a particular gene could be altered.
How does gene therapy work?
In most gene therapy studies, a "normal" gene is inserted into the genome to replace an "abnormal," disease-causing gene. A carrier molecule called a vector must be used to deliver the therapeutic gene to the patient's target cells. Currently, the most common vector is a virus that has been genetically altered to carry normal human DNA. Viruses have evolved a way of encapsulating and delivering their genes to human cells in a pathogenic manner. Scientists have tried to take advantage of this capability and manipulate the virus genome to remove disease-causing genes and insert therapeutic genes.
Target cells such as the patient's liver or lung cells are infected with the viral vector. The vector then unloads its genetic material containing the therapeutic human gene into the target cell. The generation of a functional protein product from the therapeutic gene restores the target cell to a normal state. See a diagram depicting this process.
Some of the different types of viruses used as gene therapy vectors:
Retroviruses - A class of viruses that can create double-stranded DNA copies of their RNA genomes. These copies of its genome can be integrated into the chromosomes of host cells. Human immunodeficiency virus (HIV) is a retrovirus.
Adenoviruses - A class of viruses with double-stranded DNA genomes that cause respiratory, intestinal, and eye infections in humans. The virus that causes the common cold is an adenovirus.
Adeno-associated viruses - A class of small, single-stranded DNA viruses that can insert their genetic material at a specific site on chromosome 19.
Herpes simplex viruses - A class of double-stranded DNA viruses that infect a particular cell type, neurons. Herpes simplex virus type 1 is a common human pathogen that causes cold sores.
Besides virus-mediated gene-delivery systems, there are several nonviral options for gene delivery. The simplest method is the direct introduction of therapeutic DNA into target cells. This approach is limited in its application because it can be used only with certain tissues and requires large amounts of DNA.
Another nonviral approach involves the creation of an artificial lipid sphere with an aqueous core. This liposome, which carries the therapeutic DNA, is capable of passing the DNA through the target cell's membrane.
Therapeutic DNA also can get inside target cells by chemically linking the DNA to a molecule that will bind to special cell receptors. Once bound to these receptors, the therapeutic DNA constructs are engulfed by the cell membrane and passed into the interior of the target cell. This delivery system tends to be less effective than other options.
Researchers also are experimenting with introducing a 47th (artificial human) chromosome into target cells. This chromosome would exist autonomously alongside the standard 46 --not affecting their workings or causing any mutations. It would be a large vector capable of carrying substantial amounts of genetic code, and scientists anticipate that, because of its construction and autonomy, the body's immune systems would not attack it. A problem with this potential method is the difficulty in delivering such a large molecule to the nucleus of a target cell.
What is the current status of gene therapy research?
The Food and Drug Administration (FDA) has not yet approved any human gene therapy product for sale. Current gene therapy is experimental and has not proven very successful in clinical trials. Little progress has been made since the first gene therapy clinical trial began in 1990. In 1999, gene therapy suffered a major setback with the death of 18-year-old Jesse Gelsinger. Jesse was participating in a gene therapy trial for ornithine transcarboxylase deficiency (OTCD). He died from multiple organ failures 4 days after starting the treatment. His death is believed to have been triggered by a severe immune response to the adenovirus carrier.
Another major blow came in January 2003, when the FDA placed a temporary halt on all gene therapy trials using retroviral vectors in blood stem cells. FDA took this action after it learned that a second child treated in a French gene therapy trial had developed a leukemia-like condition. Both this child and another who had developed a similar condition in August 2002 had been successfully treated by gene therapy for X-linked severe combined immunodeficiency disease (X-SCID), also known as "bubble baby syndrome."
FDA's Biological Response Modifiers Advisory Committee (BRMAC) met at the end of February 2003 to discuss possible measures that could allow a number of retroviral gene therapy trials for treatment of life-threatening diseases to proceed with appropriate safeguards. FDA has yet to make a decision based on the discussions and advice of the BRMAC meeting.
What factors have kept gene therapy from becoming an effective treatment for genetic disease?
Short-lived nature of gene therapy - Before gene therapy can become a permanent cure for any condition, the therapeutic DNA introduced into target cells must remain functional and the cells containing the therapeutic DNA must be long-lived and stable. Problems with integrating therapeutic DNA into the genome and the rapidly dividing nature of many cells prevent gene therapy from achieving any long-term benefits. Patients will have to undergo multiple rounds of gene therapy.
Immune response - Anytime a foreign object is introduced into human tissues, the immune system is designed to attack the invader. The risk of stimulating the immune system in a way that reduces gene therapy effectiveness is always a potential risk. Furthermore, the immune system's enhanced response to invaders it has seen before makes it difficult for gene therapy to be repeated in patients.
Problems with viral vectors - Viruses, while the carrier of choice in most gene therapy studies, present a variety of potential problems to the patient --toxicity, immune and inflammatory responses, and gene control and targeting issues. In addition, there is always the fear that the viral vector, once inside the patient, may recover its ability to cause disease.
Multigene disorders - Conditions or disorders that arise from mutations in a single gene are the best candidates for gene therapy. Unfortunately, some the most commonly occurring disorders, such as heart disease, high blood pressure, Alzheimer's disease, arthritis, and diabetes, are caused by the combined effects of variations in many genes. Multigene or multifactorial disorders such as these would be especially difficult to treat effectively using gene therapy. For more information on different types of genetic disease, see Genetic Disease Information.
What are some recent developments in gene therapy research?
University of California, Los Angeles, research team gets genes into the brain using liposomes coated in a polymer call polyethylene glycol (PEG). The transfer of genes into the brain is a significant achievement because viral vectors are too big to get across the "blood-brain barrier." This method has potential for treating Parkinson's disease. See Undercover genes slip into the brain at NewScientist.com (March 20, 2003).
RNA interference or gene silencing may be a new way to treat Huntington's. Short pieces of double-stranded RNA (short, interfering RNAs or siRNAs) are used by cells to degrade RNA of a particular sequence. If a siRNA is designed to match the RNA copied from a faulty gene, then the abnormal protein product of that gene will not be produced. See Gene therapy may switch off Huntington's at NewScientist.com (March 13, 2003).
New gene therapy approach repairs errors in messenger RNA derived from defective genes. Technique has potential to treat the blood disorder thalassaemia, cystic fibrosis, and some cancers. See Subtle gene therapy tackles blood disorder at NewScientist.com (October 11, 2002).
Gene therapy for treating children with X-SCID (sever combined immunodeficiency) or the "bubble boy" disease is stopped in France when the treatment causes leukemia in one of the patients. See 'Miracle' gene therapy trial halted at NewScientist.com (October 3, 2002).
Researchers at Case Western Reserve University and Copernicus Therapeutics are able to create tiny liposomes 25 nanometers across that can carry therapeutic DNA through pores in the nuclear membrane. See DNA nanoballs boost gene therapy at NewScientist.com (May 12, 2002).
Sickle cell is successfully treated in mice. See Murine Gene Therapy Corrects Symptoms of Sickle Cell Disease from March 18, 2002, issue of The Scientist.
What are some of the ethical considerations for using gene therapy?
--Some Questions to Consider...
What is normal and what is a disability or disorder, and who decides?
Are disabilities diseases? Do they need to be cured or prevented?
Does searching for a cure demean the lives of individuals presently affected by disabilities?
Is somatic gene therapy (which is done in the adult cells of persons known to have the disease) more or less ethical than germline gene therapy (which is done in egg and sperm cells and prevents the trait from being passed on to further generations)? In cases of somatic gene therapy, the procedure may have to be repeated in future generations.
Send me an e-mail
More Pictures
guess whats new technique |
advantages of biotechnology
UPCOMING FIELDS
ANTISENSE TECHNOLOGY
NEUROBIOLOGY
RNA INFERENCE
KNOCK OUT GENES
CHROMOSOMAL WALKING
DNA SEQUENCING
venkatesh.perikala@gmail.com |

